

By Christine Monahan and Sabrina Corlette. This blog originally appeared on The Commonwealth Fund Blog on August 22, 2013 and is reproduced here in its entirety.
The Affordable Care Act brings a number of much-needed reforms to the private health insurance market, particularly for individuals and small employers. Many of the most significant changes preventing insurers from excluding people from coverage based on preexisting conditions or using health status and gender to set premiums, as well as requiring insurers to cover a comprehensive set of benefits—take effect for plan years beginning on or after January 1, 2014. However, some insurers have begun encouraging their customers to renew their coverage ahead of schedule—in December 2013 or sooner. This way, the insurer can delay implementing the Affordable Care Act’s reforms for up to 12 months.
What’s at Stake? Over the long term, early renewals will negatively impact everyone, but young, healthy, and male consumers could financially gain from it in the short term. Insurers are offering healthy and younger individuals and small businesses favorable rates to renew their policies in 2013 instead of 2014. Those who do so will be carved out of the risk pool for the new marketplace in 2014. Yet it is young, healthy people that the new marketplace needs in 2014 to keep premiums affordable. If the only people who enroll in new plans in 2014 are more expensive to cover than insurers have accounted for in setting their rates—which have been coming in lower than anticipated in a number of states—insurers will need to make up for the higher risk the following year. That means higher premiums for everyone in 2015.
Early renewals are also likely to breed even more confusion than already exists about what the Affordable Care Act does, and when its rules go into effect. Consumers may not understand all the new benefits they may give up if they renew early. Indeed, some insurers are asking policyholders to decide to renew before state health insurance marketplaces go live, meaning they won’t have an opportunity to compare their current plan with the new marketplace options.
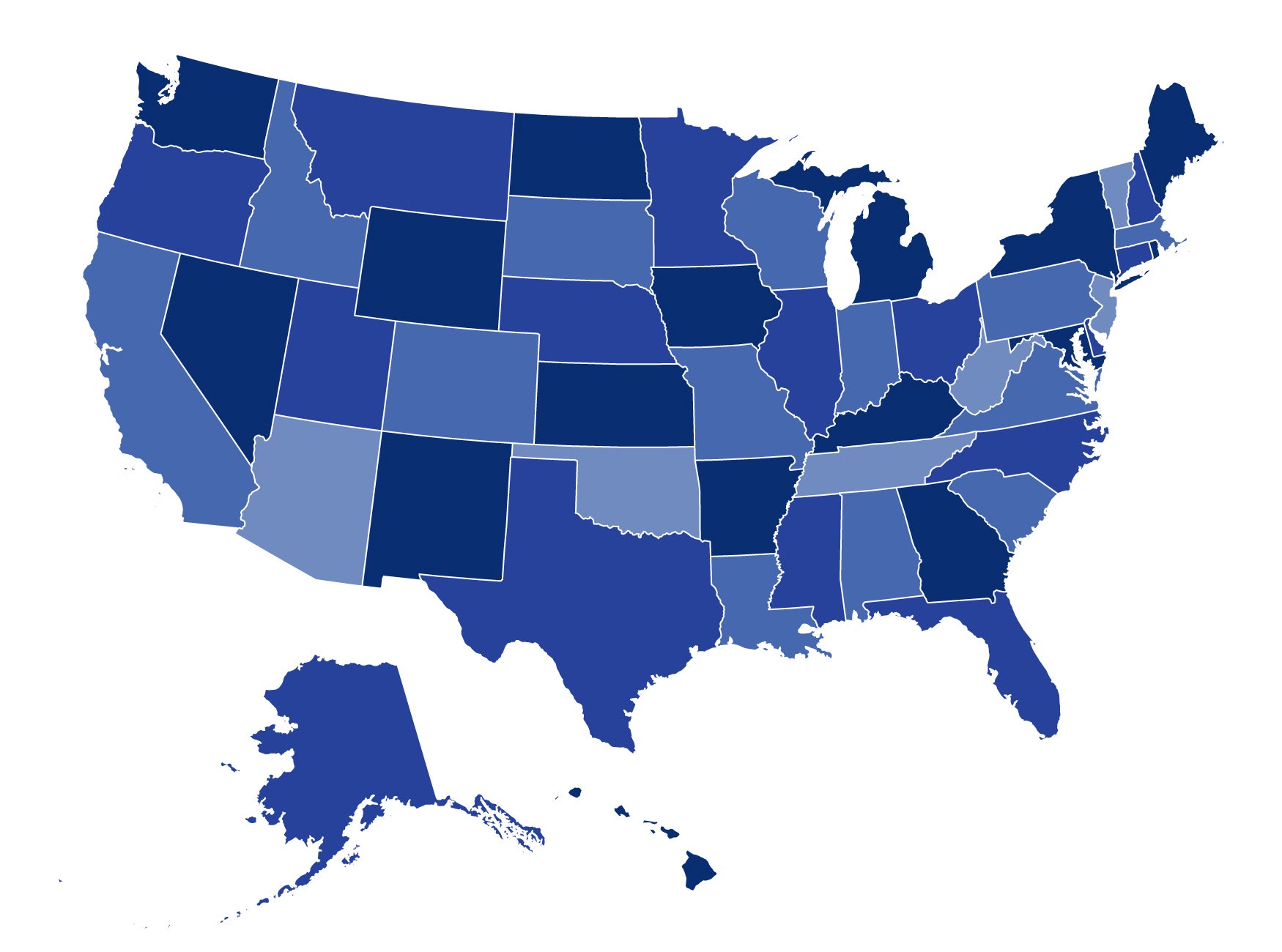
State Action. While the Obama Administration has not published any guidance on early renewals, some states are stepping up to prohibit or limit the practice.
Three states have prohibited early renewals in both individual and small-group markets. In explaining its ban, Missouri referred to language in the state insurance code specifying that renewals cannot occur more than once a year, while Illinois and Rhode Island informed insurers that they would withhold approval from forms for early renewal products. Illinois reasoned that early renewing “violate[s] the spirit and intent of the law that the market reforms be administered in a consistent and timely manner,” and Rhode Island officials cited concerns about discrimination and questioned the financial soundness of extending current rates for early renewal products without adjusting for additional costs, such as medical inflation and new taxes and fees.
Three other states have banned early renewals in only certain markets. New York passed new legislation prohibiting early renewals in the small-group market. Washington outlawed early renewals by association health plans, while soliciting public comment on action in its traditional individual and small-group markets. California has made terminating all non-ACA compliant individual policies by December 31, 2013 a condition for insurer participation in its individual exchange.
Massachusetts and Oregon took a different approach, requiring individual market policies issued in 2013 to end no later than March 31, 2014. While not prohibiting early renewals explicitly, this approach makes taking advantage of the loophole less attractive because insurers’ plans will have to come into compliance with the ACA market reforms by April 1, 2014.
Other states issued guidance permitting early renewals, but set rules for the practice and, in some cases, explicitly cautioned insurers about how they proceed. Idaho and Kentucky, for example, expressed concern that early renewals may be discriminatory and required insurers offering early renewals to make the option available to all current policyholders. Montana set similar rules to prevent discrimination and prohibited insurers from charging higher premiums for early renewal policies that offer substantially similar benefits and cost-sharing as the pre-renewal policy. Other states, including Arkansas and Colorado, established notification requirements to help ensure that consumers understand all of their options and insurers are not using early renewals to risk select. However, these rules may not be enough to prevent discriminatory marketing practices that encourage certain policyholders—particularly those that are younger, healthier, and male—to renew early and others to wait until January 2014.
What’s Next? A narrow window of opportunity still exists for states to close this loophole. Even without passing new legislation, states have a number of tools at their disposal, including existing rules regarding the length of plan years or frequency of renewals, unfair trade practice and nondiscrimination laws, and rating and solvency requirements. States that prohibit or limit early renewals will ensure that consumers don’t have to wait an extra year to get the full range of protections under the Affordable Care Act, and will help keep premiums down over the long run.
2 Comments
This is an interesting take on the early renewal conundrum.
I’m currently working with a carrier that is offering an early renewal option based on their customers’ next renewal dates. This carrier reluctantly made the decisions to offer early renewals at the insistence of its small group customers and their brokers.
The group customers stand to benefit by delaying the transition of their medical products to the ACA-compliant products. For this carrier’s small group customers, the biggest change is associated with their total premium: The move from today’s composite rating to tomorrow’s member-level build-up presents a significant premium risk for small groups. The groups will struggle to adjust their expectations to the broad variations in a given family’s premium as well as a group’s total premium. Today’s rating mechanism makes it simple to add the employees’ premium costs based on the selected coverage level. Tomorrow’s member-level build-up mechanism and its cumbersome rules will challenge most small businesses to estimate and understand their potential spend on employee premiums. Delaying this shock with an opportunity for an additional 11 months to learn from other businesses is advantageous.
In regards to early renewals impacting the risk pool and thus the 2015 rates, I think this risk is actually higher for 2016. Carriers will be required to submit their 2015 products and rates in April/May of 2014, and will likely be making similar guesstimates that they needed to make this year. The carrier’s actuaries simply will not have enough real data to support their pricing process. It will be in April/May of 2015 as carriers price and submit their 2016 plans that there’s a risk of using a full set of skewed data from 2014.
However, by the time the calendar clicks into 2015, the carriers and regulators will have already re-focused on the 2016 expansion of small group from 50-and-under employees to 100-and-under employees so perhaps attempting to forecast the industry’s highest priority issues more than 18 months out isn’t very advisable.
I called Kaiser to see if they offer early renewal and if I can keep my current plan, and they said no, so I’m very disappointed. My current plan is being canceled. The only requirement it doesn’t meet is rx coverage, but it’s SOOOOO much better in a great many other ways than the plan I am being offered that meets all ACA minimum requirements, not to mention the premium now is lower than it will be for the new/worse plan. I was told by Kaiser today that a plan that is comparable to my current $426 plan (except the new will have rx coverage) will be $811 per month.
13 Trackbacks and Pingbacks