

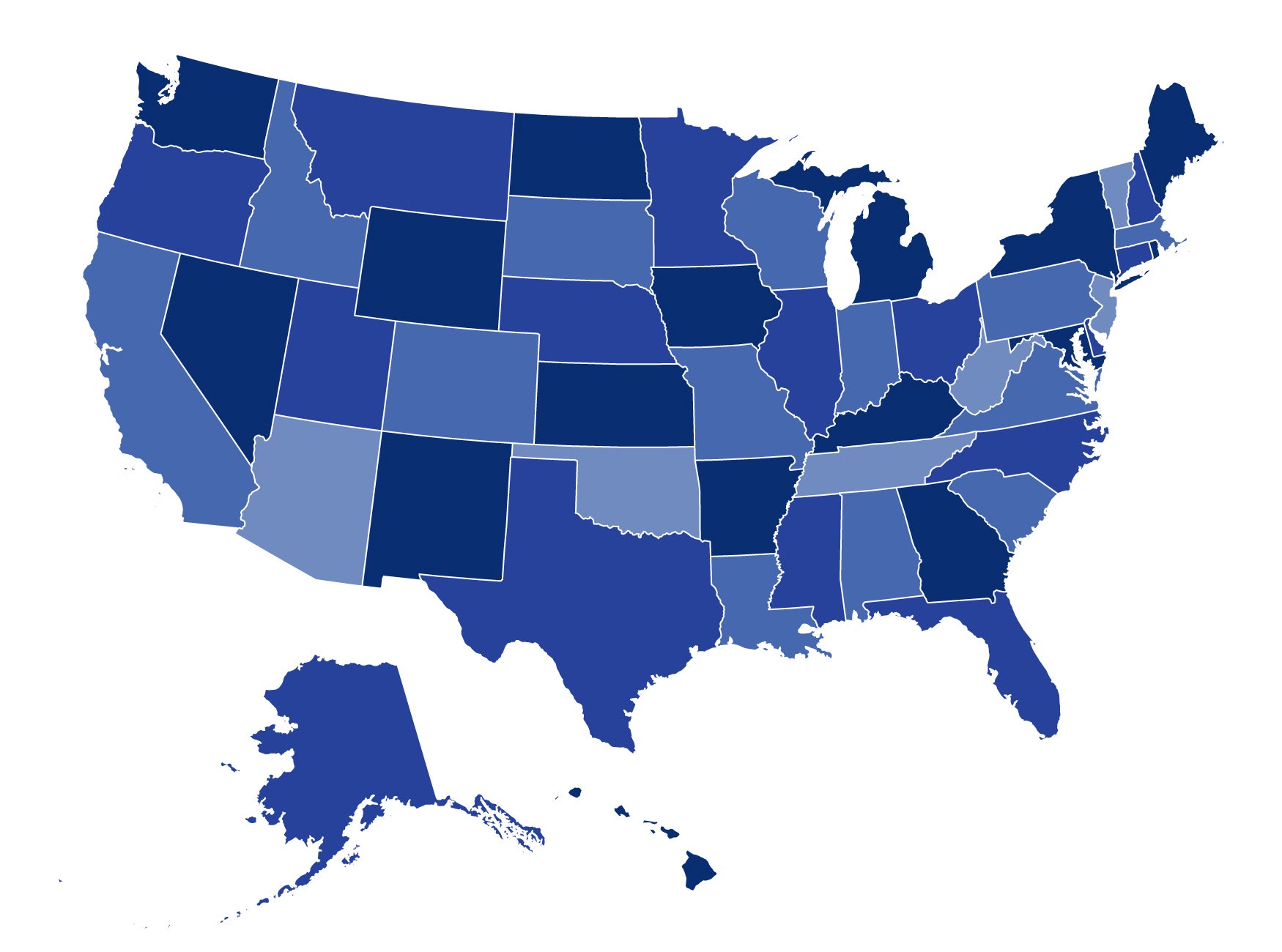
In our latest issue brief for the Commonwealth Fund, we examine states’ efforts to implement the Affordable Care Act’s requirement that health plans cover a minimum set of essential health benefits (EHB). We found that 24 states and the District of Columbia selected the EHB benchmark plan for their states and 26 states made no selection. Of those selecting a plan, 19 chose one of their largest small-group plans. Under federal rules, states that did not make a selection will default to the largest small-group plan in their state. As a result, only five states will not have an existing small-group plan as their EHB benchmark.
Our report concludes that, by selecting existing small-group plans, federal and state officials will help ensure a smoother transition into the new marketplaces and an easier adjustment to new coverage. In 2014, the health plans covering the EHB will look very similar to those in the small group marketplace today.
Our report also found that states took diverse approaches to selecting a benchmark plan, with many launching novel, inter-governmental decision-making processes that engaged stakeholders through public meetings, advisory groups, and task forces. However, other states did little to educate the public and seek input, and only a few published important plan documents that would permit stakeholders and citizens to fully compare their options (although many published plan summaries).
The U.S. Department of Health and Human Services has said that the state benchmark approach will be a transitional, two-year policy, giving federal and state officials an opportunity to monitor its effectiveness and impact on consumers and small-business purchasers. Our report concludes that, should HHS consider maintaining a policy of state-based benchmarks, they should consider establishing minimum standards for changing or updating states’ benchmark selections, such as by requiring an open, public process and the publication of full plan documents.
In addition, our interviews with state officials revealed important implementation questions that could impact consumers’ ability to obtain the full range of benefits they have been promised under the ACA. These questions relate to states’ enforcement authority, the lack of time for a robust review of insurers’ policies, the addition of supplemental benefits, particularly habilitation services, and whether to allow insurers to substitute coverage of items and services, so long as the new items or services covered are actuarially equivalent to those being replaced.
This brief is the latest in our Implementing the Affordable Care Act series, supported by The Commonwealth Fund. In past briefs we’ve covered state action on the ACA’s 2014 market reforms, child-only coverage, and the early market reforms. For updates on these and other health insurance reform issues, stay tuned to CHIRblog!
1 Trackback or Pingback