


By Dania Palanker, Georgetown University Center on Health Insurance Reforms and Edwin Park, Georgetown University Center for Children and Families
The Fifth Circuit Court of Appeals has asked the parties in Texas v. United States to file supplemental briefings on the issue of whether the defendant states attorneys generals and the U.S. House of Representatives have standing to appeal. Standing is a legal term that means a party has a right to bring a lawsuit, intervene in a lawsuit, and/or bring an appeal. To have standing, a party needs to show an injury or actual harm and, if an intervenor rather than original party to the suit, show that they intervened in a timely manner. In this instance, the appeals court is considering whether any of the intervenors have the right to appeal the decision from last December that found the entire Affordable Care Act (ACA) unlawful. The notion that the defendant states, led by California, would not experience harm if the ACA is invalidated, seems absurd. The court’s decision in this case will affect every American, including the 158.6 million who live in the intervening states.
Oral arguments for the appeal of a lower court decision for Texas v. United States will be heard on Tuesday, July 9, 2019 at the Fifth Circuit Court of Appeals. The case was brought in a Texas court and claims that the individual mandate is unconstitutional following the elimination of the tax penalty, as the Supreme Court previously upheld the mandate under Congress’ taxing power. In addition, the plaintiffs claim the entire ACA should be invalidated because it is not severable from the rest of the law. State attorneys general intervened to defend the law since the Department of Justice is arguing the same side as the plaintiffs. In December, Judge Reed O’Connor delivered a judgment that the mandate is unconstitutional and struck down the entire law, but he also issued a stay as the decision is appealed, so the ACA remains in effect. However, the case threatens all the coverage expansions and consumer protections in the ACA. After the appeal to the Fifth Circuit, the U.S. House of Representatives and four states joined as additional intervenors.
The 21 States Have a Huge Financial Interest in Upholding the ACA
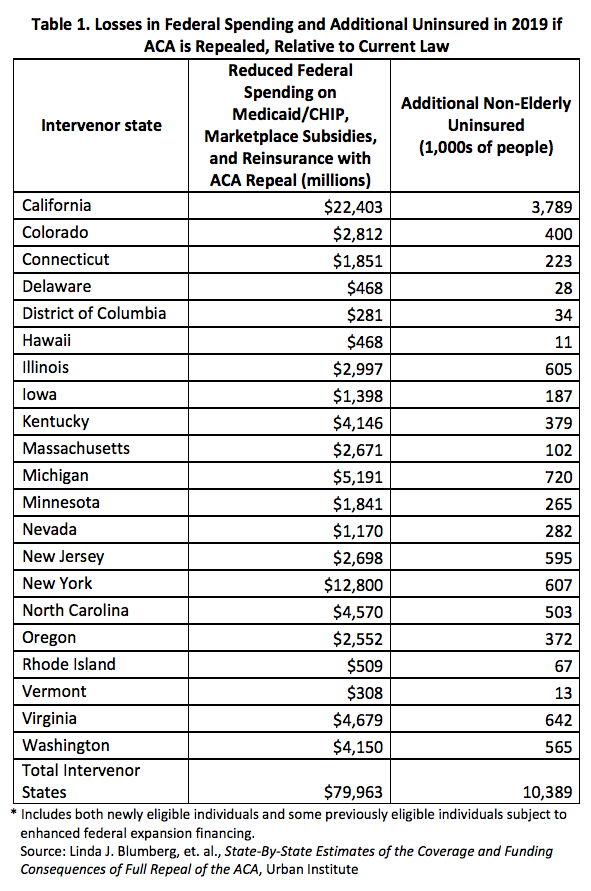
The 21 intervenor states have a clear financial interest in defending the ACA. If the ACA is repealed, intervenor states[1] will lose about $702 billion in federal funds over ten years, including a loss of $518 billion from the elimination of the federal insurance marketplaces and Medicaid expansion funds. See Table 1. This loss of funding has a snowball effect. The funding that comes into the states pays for health coverage for the states’ residents. Following implementation of the coverage expansions, the uninsured rate for adults ages 19-64 dropped from 24 percent to just 10 percent in California. Similar drops were seen in the other intervenor states. In total, nearly 4.8 million residents of the intervenor states would lose marketplace coverage and over 9.2 million could lose Medicaid expansion coverage, because they are eligible only because of the Medicaid expansion, in the intervenor states. This does not include young adults under age 26 that will lose coverage under a parent’s employer-based plan. As people lose coverage, health providers lose important revenue that provides jobs and other economic advantages to the states. In California alone, there would be over $140 billion more in uncompensated care over ten years. Hospitals could lose about $64 billion in revenue and physicians could lose over $24 billion.1
The ACA Improves the Health and Well-Being of Residents of the 21 States
The ACA’s benefit to the states is more than just federal funding. Since the implementation of the ACA, 18 of the 21 intervenor states have improved in state health system performance. While the ACA is not necessarily the direct cause of these improvements, many of the ACA protections have increased access to health care services, particularly for lower income populations, and the ACA encouraged delivery system reforms to improve quality of care. Private insurance and Medicaid expansion are just two areas where the ACA has helped to improve access to care and the health of state residents.
Private Insurance Improvements
As many as 51 percent of non-elderly Americans that have a preexisting condition can no longer be discriminated against by health insurance companies for their condition, either by having claims denied, being denied coverage altogether, or charged more in premiums than healthier people. Guaranteed coverage of preventive services without cost-sharing has improved access to services such as vaccines, cancer screenings, and prenatal care for over 74.9 million people in the intervenor states. A maximum out-of-pocket means health insurance plans are limited in the amount any member has to pay towards covered, in-network claims. Annual and lifetime limits have become a thing of the past, so that insurance no longer leaves those with the most costly illnesses or conditions suddenly without coverage. But about 12 million people who have an out-of-pocket cap and about 53.3 million people who have no lifetime or annual limits in the intervenor states because of the ACA would lose these protections against limits if the ACA is overturned. In addition, the ACA’s minimum essential health benefits are critical to the public health infrastructure in the states, by improving access to care in the event of an infectious disease outbreak, combating the opioid crisis, and delivering mental health services to vulnerable populations. Further, all individual and small group market plans must cover maternity coverage, promoting healthier pregnancies and better access to pre- and postnatal care during a time of a maternal mortality crisis.
Medicaid Expansion and Improvements
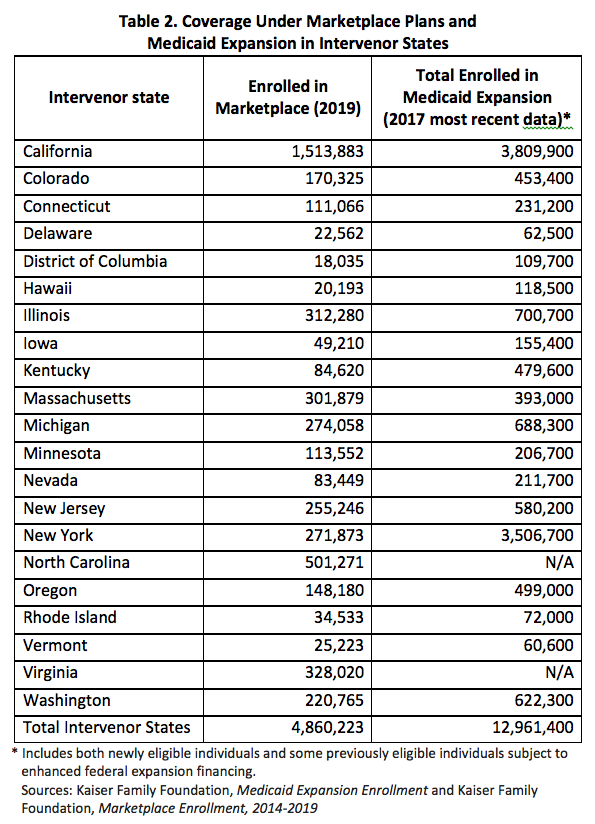
The Kaiser Family Foundation has conducted a comprehensive review of the research literature — evaluating more than 200 studies — finding a wide array of benefits of the Medicaid expansion. Twenty of the 21 intervenor states have expanded Medicaid, covering almost 13 million. See Table 2. States adopting the Medicaid expansion saw significant health coverage gains and reductions in the uninsured rates. The Medicaid expansion also resulted in greater access to needed care including greater use of preventive care and cancer diagnosis testing, increased access to needed medications including treatment for opioid use disorder, improvements in health disparities, higher quality of care and shorter hospital stays. Rural areas saw disproportionate coverage gains and increased access to needed care. Research also shows that increased coverage of low-income parents raises participation among their children eligible for Medicaid and the Children’s Health Insurance Program.
Following implementation of the expansion, studies found the expansion led to improvements in self-reported health status, improved outcomes for cardiac surgery patients, and reductions in maternal and infant mortality. Among low-income individuals, the expansion was also associated with significant reductions in out-of-pocket medical costs, declines in problems affording care, fewer unpaid medical bills and debt sent to third-party collection agencies, and reduced risk of personal bankruptcy. Hospitals, clinics and other providers experienced sizable reductions in uncompensated care. In addition, expansion states obtained substantial offsetting savings in other parts of their budgets including lower state costs related to behavioral health and other services provided to previously uninsured individuals and the criminal justice system.
The ACA included numerous other Medicaid improvements. That includes, among others, simplification of the eligibility and enrollment procedures to increase participation among eligible individuals and families, expanded eligibility and greater access to long-term services and supports, coverage of former foster youth through age 26, delivery system reforms to better coordinate and improve quality of care, and increased discounts paid by drug manufacturers to make outpatient prescription drug costs more affordable for state Medicaid programs
Conclusion
There is no doubt that the intervenor states have a lot of money to lose if the ACA is repealed. But, beyond money, these states face the loss of health coverage, programs and services that help to improve access to care and ultimately the overall health of their residents. The recent request for a briefing on standing by the Fifth Circuit does not signal the position of the court. The judges may simply want to ensure that they are considering all aspects of an important case that affects all Americans as comprehensively as possible. And in doing so, they should consider all the ways the ACA benefits the intervenor states, as well as the risk to those states and their residents of repeal.
[1] This data is based on a 2018 declaration provided to the court by Henry Aaron, a Senior Fellow at the Brookings Institution. The estimates are based on a 2019-2028 budget window; any court decision will now affect 2020 and later.
3 Trackbacks and Pingbacks