

State and federal insurance regulators increasingly recognize that transgender exclusions contravene scientific evidence, best medical practice, and legal standards that prohibit discrimination on the basis of gender identity. In 2014, for instance, Medicare overturned its three-decades-old transgender exclusion, and the U.S. Department of Health and Human Services (HHS) Office for Civil Rights issued a proposed rule that is expected to ban transgender exclusions in many private health plans and state Medicaid plans nationwide. The road to these changes, however, has been paved by state insurance regulators who have taken action to prohibit insurance exclusions that discriminate on the basis of gender identity.
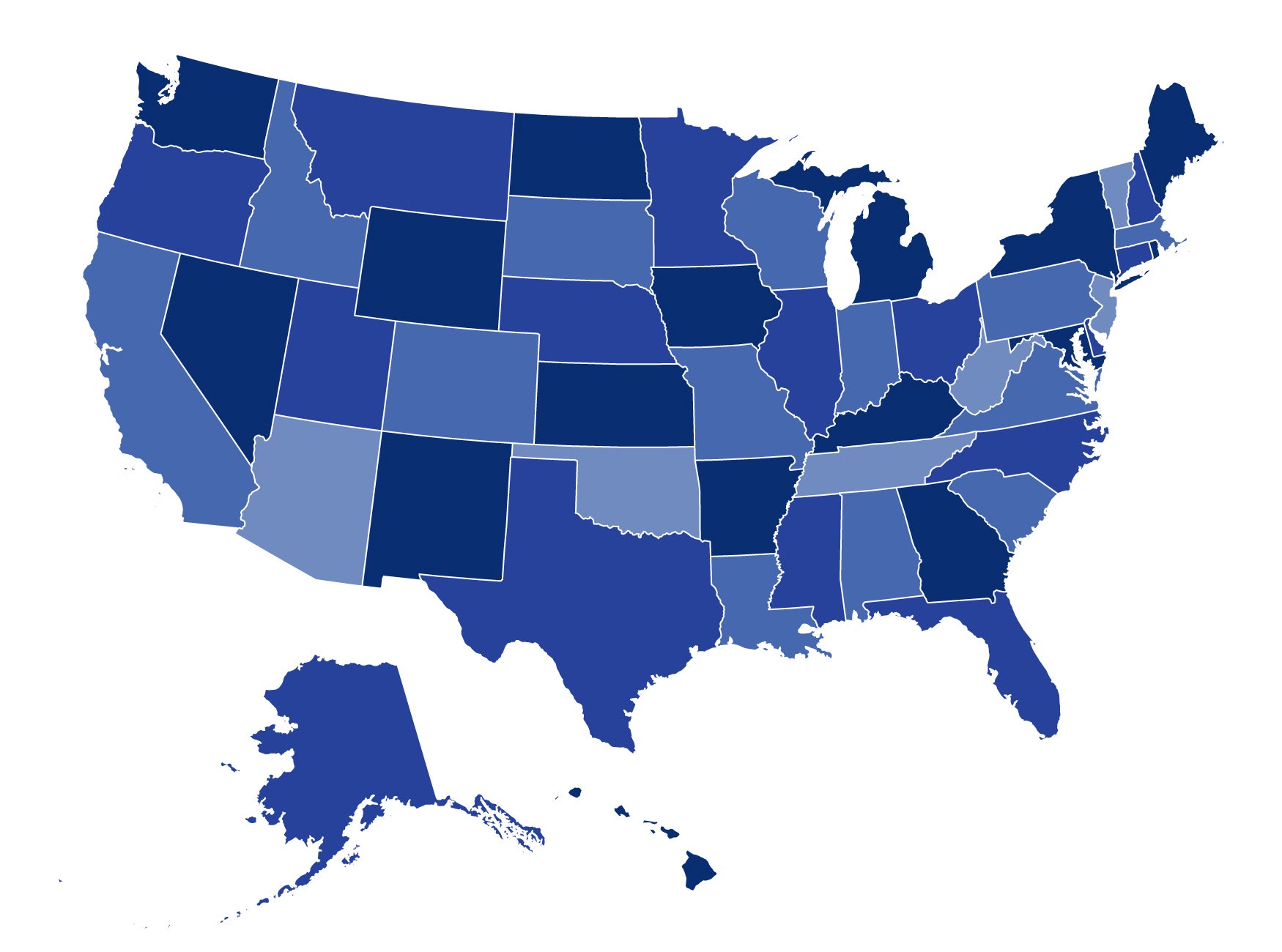
In March 2013, only three states and DC had prohibited transgender exclusions; today, 15 states and DC have done so. These states are California, Colorado, Connecticut, Delaware, District of Columbia, Illinois, Maryland, Massachusetts, Michigan, Minnesota, New York, Nevada, Oregon, Rhode Island, Vermont, and Washington. Similar guidance is under consideration by regulators in other states and expected imminently.
Although each state varies in its reasoning, nearly every bulletin relies on state laws on unfair trade practices, sex or gender identity nondiscrimination, or mental health parity as a basis for prohibiting transgender exclusions. Some, but not all, also reference federal law, including Section 1557 of the Affordable Care Act; the essential health benefit nondiscrimination protections; and the Mental Health Parity and Addiction Equity Act.
There is significant momentum to address transgender exclusions—the guidance from Delaware was issued last week following a recent Michigan bulletin on form review requirements—and state guidance is particularly timely ahead of 2017 filing deadlines and full implementation of Section 1557 of the Affordable Care Act. State regulators are also addressing transgender exclusions via form filing guidance, form review checklists, and insurer attestations.
Transgender exclusions discriminate by arbitrarily singling out the transgender population for categorical denials of coverage for benefits otherwise provided to non-transgender people. Like anyone, transgender people need preventive care to stay healthy and acute care when they become sick. Some may also need medical treatment to physically transition from the sex they were assigned at birth (the gender on their original birth certificate) to the gender with which they identify. This care is frequently referred to as “transition-related care” and may include mental health counseling, hormone therapy, and surgeries.
Expert medical organizations—including the American Medical Association and the American Psychological Association, among many others—agree that transition-related care is medically necessary for transgender people. And gender dysphoria (the medical diagnosis that is frequently used to describe a transgender identity) is explicitly described in the American Psychiatric Association’s Fifth Edition of the Diagnostic and Statistical Manual of Mental Disorders, known as the DSM-5.
Unfortunately, many plans continue to use categorical benefit exclusions that deny coverage for any service relating to gender transition. Insurers have invoked these exclusions to, for instance, deny coverage to transgender individuals for a wide range of basic health care services, including setting a broken arm and providing preventive screenings that are traditionally considered to be gender-specific (such as prostate exams or mammograms). These denials occur even though these services are not unique to transgender individuals and are routinely covered for non-transgender people on the same plan.
Transgender exclusions are still common in state-regulated plans: they were included in the 2017 essential health benefits base-benchmark plans in 43 states and can be found in all markets in many states. These exclusions persist even though all major insurers have designed products that do not contain transgender exclusions to accommodate private sector demand for inclusive coverage.
At the same time, the removal of transgender exclusions does not impose significant costs. This is because the transgender population is relatively small—there are an estimated 700,000 transgender people in the United States—and because cost and utilization is low. Indeed, actuarial projections frequently adopt inaccurate assumptions about the cost and utilization of transition-related care.
The City of San Francisco, for example, dramatically overestimated the cost of removing transgender exclusions from its employee health plan. The City initially imposed a small rider that resulted in a substantial surplus after the city collected $5.6 million and paid out only $386,417 on 37 claims from 2001 to 2006. The city dropped the rider in 2006 and has since covered transition-related care as part of its core benefit package.
The California Department of Insurance similarly compared the costs and benefits of California’s law that prohibited insurance discrimination against transgender people. The Department found an “immaterial” impact on premium costs, and “the benefits of eliminating discrimination far exceed the insignificant costs” because of improved health outcomes for transgender people. Other studies have similarly found the removal of transgender exclusions to be highly cost-effective with low utilization but significant benefits for enrollees and plans.
Despite the long history of insurance discrimination against transgender people, there is growing federal, state, and private sector momentum to remove discriminatory transgender exclusions. State regulators should consider joining these 15 states and DC in taking action to ban transgender exclusions from state-regulated coverage.
1 Comment
Katie, CHIR,
Thank you for the well reasoned post, which reflects the scientific reality in the 21st Century that medically supervised transition care for individuals who are transgender or gender non-conforming is medically necessary, safe, and effective. We know that people living as their authentic selves are more healthy and productive. The science also now shows that children with gender dysphoria receiving medically supervised care achieve nearly identical health and productivity outcomes as adults as their cisgender peers.
Exclusions of coverage for this medical care are based on 20th century beliefs no longer supported by nearly every medical professional organization, or the science itself.
Plus, it’s wonderful to be a part of the Washington, DC community, which leads the nation in protecting the opportunity of every LGBTQ resident to achieve their life goals through optimal health.
Our job as a medical profession is to provide the best evidence-based, medically supported care to so that every human produces optimal health for themselves and their families/communities; it’s what we came into medicine to do.
Best,
Ted Eytan, MD, MS, MPH
Family Physician
Medical Director, Kaiser Permanente Center for Total Health
Washington, DC, USA
3 Trackbacks and Pingbacks